THE PROBLEM OF NON-ADHERENCE
What is non-adherence?
Adherence to a medication regimen is defined as “the extent to which patients take their medications as prescribed by their healthcare providers.”[1]
Poor adherence or non-adherence to medications includes all patients who do not commence their prescribed therapy at all, discontinue it prematurely, or take their medications in doses or frequencies different from the prescribing clinician’s recommendations. The treatment of chronic illnesses commonly includes the long-term use of pharmacotherapy. Although these medications are effective in combating disease, their full benefits can often not be realized, as approximately 50% of all patients with chronic conditions do not take their medications as prescribed[2]. To put this into perspective, even though it is well known that antidiabetics, antihypertensive, and lipid-lowering medication therapies can significantly reduce the risk of ischemic events[3] [4] [5], long-term adherence to these medications is poor even among patients who have already experienced a cardiovascular event[6]. With regards to hypertension, even though pharmacological antihypertensive therapy has a positive safety and tolerability profile and reduces the risk of stroke by approximately 30% and myocardial infarction by approximately 15%[5], evidence from several studies suggests that as many as 50% to 80% of patients are non-adherent to their antihypertensive treatment regimen[7].
What are the consequences of non-adherence?
In general, non-adherence leads to poor disease control with a burden on patient quality of life and healthcare systems[8], whereas patients who take their prescribed medications regularly are more likely to enjoy better health outcomes, avoid complications and premature death, and use less of emergency care and inpatient hospital services[9].
Medication non-adherence leads to premature deaths as well as an increased use of healthcare services. In the United States, between USD 100 and 300 billion of avoidable health care costs and approximately 125’000 deaths have been attributed to non-adherence per year[10] [11]. These estimates do not include avoidable costs of long-term care, diagnostic testing and pharmacy costs related to therapy intensification. Broader societal costs of increased disability, reduced productivity, and sick leave are also not considered[10].
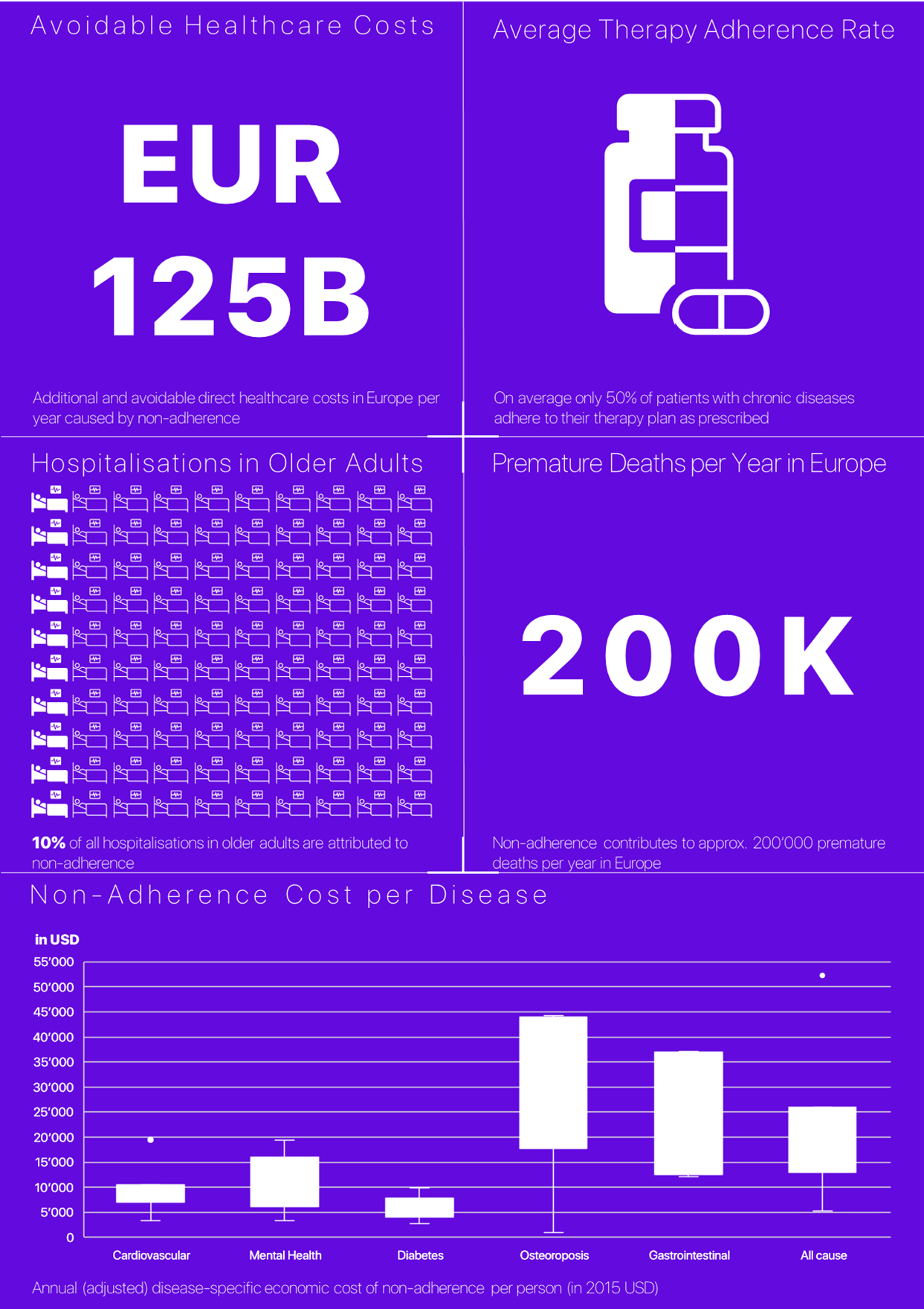
With regards to Europe, it is estimated that non-adherence contributes to nearly 200’00 premature deaths per year[9] and costs European governments EUR 125 billion annually in excess healthcare services[12]. Diabetes, hypertension, and hyperlipidemia appear to give rise to the highest avoidable costs. Among patients with these three conditions, it has been estimated that between 4% and 31% do not fill their first prescription. Of those who do fill their prescription, only 50% to 70% take their medications regularly (i.e., at least 80% of the time)[9]. Additionally, 10% of hospitalizations in older adults are attributed to medication non-adherence[13] [14]. Ever since the WHO report on adherence was published, many interventional studies have been conducted, but adherence rates have not noticeably improved[15] [16]. The Collabree infographic below shows the most important stats.
What are the consequences per indication?
A variety of different studies have examined the costs associated with poor therapy adherence. To get an overview of their results, a comprehensive literature search was conducted by PubMed and Scopus in September 2017[17]. 79 individual studies assessing the cost of non-adherence across different disease groups were included. Across these studies, a many different indicators (35 in total) were used to measure the cost of non-adherence and 19 reporting styles were identified. Because of the resultant heterogeneity of approaches to the estimation of costs or levels of adherence it is not surprising that cost estimates for non-adherence spanned wide ranges.
Their conclusions suggested that the annual (adjusted) disease-specific economic cost of non-adherence per person ranged from USD 949 to USD 44’190 (converted to 2015 USD). Costs attributed to ‘all causes’ non-adherence ranged from USD 5’271 to USD 52’341[17].
The reason why we founded Collabree
Although this systematic review of existing research was unable to provide a clear indication of the exact non-adherence costs per disease, it leaves no doubt that the economic, clinical, and humanistic consequences of therapy non-adherence are already enormous and will continue to grow as the burden of chronic diseases increases worldwide. There is an immense opportunity for both major cost savings in healthcare systems and improving patient’s health outcomes. We can achieve both by reimagining adherence interventions for patients with chronic conditions.
Most existing interventions fail to consider fundamental insights from modern science about how we behave. Our mission is to leverage these insights to make behavior change as easy as 1-2-3. We strive to provide our users the most motivating, fun, and inspiring behavioral intervention so they can easily establish sustainable and sticky habits to follow their therapy plans.
Find out more how Collabree can help improve patients’ outcomes
Learn more about Collabree’s digital intervention and how we can help you or your patients with the difficult task of behavior change and establishing sticky habits. Get in touch here:
Pascal Kurz
CEO – Collabree AG
[email protected]
Literature
[1]: Osterberg, L. & Blaschke, T. Adherence to medication. New England Journal of Medicine 353, 487–497 (2005). [2]: World Health Organization. Adherence to long-term therapies - Evidence for action. (2003). [3]: Amarenco, P. & Labreuche, J. Lipid management in the prevention of stroke: review and updated meta-analysis of statins for stroke prevention. The Lancet Neurology 8, 453–463 (2009). [4]: Baigent, C. et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet 366, 1267–1278 (2005). [5]: Law, M. R., Morris, J. K. & Wald, N. J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ (Clinical research ed.) 338, b1665–b1665 (2009). [6]: Glader, E. L., Sjölander, M., Eriksson, M. & Lundberg, M. Persistent use of secondary preventive drugs declines rapidly during the first 2 years after stroke. Stroke 41, 397–401 (2010). [7]: Brown, M. T. & Bussell, J. K. Medication adherence: WHO cares? Mayo Clinic Proceedings 86, 304–314 (2011). [8]: Schroeder, K., Fahey, T. & Ebrahim, S. Interventions for improving adherence to treatment in patients with high blood pressure in ambulatory settings. Cochrane Database of Systematic Reviews (2004) doi:10.1002/14651858.cd004804. [9]: Khan, R. & Socha-Dietrich, K. Investing in medication adherence improves health outcomes and health system efficiency. (2018). [10]: Iuga, A. O. & McGuire, M. J. Adherence and health care costs. Risk Management and Healthcare Policy 7, 35–44 (2014). [11]: Viswanathan, M. et al. Interventions to Improve Adherence to Self-administered Medications for Chronic Diseases in the United States: A Systematic Review. Annals of Internal Medicine 157, 785–795 (2012). [12]: European Comission; OECD. Health at a glance: Europe 2018 - State of health in the EU cycle. (2018). doi:10.1787/f222b050-mt. [13]: Sokol, M. C., McGuigan, K. A., Verbrugge, R. R. & Epstein, R. S. Impact of Medication Adherence on Hospitalization Risk and Healthcare Cost. Medical Care 43, (2005). [14]: Vermeire, E., Avonts, D., van Royen, P., Buntinx, F. & Denekens, J. Context and health outcomes. The Lancet 357, 2059–2060 (2001). [15]: Naderi, S. H., Bestwick, J. P. & Wald, D. S. Adherence to drugs that prevent cardiovascular disease: Meta-analysis on 376,162 patients. American Journal of Medicine 125, 882-887.e1 (2012). [16]: Briesacher, B. A., Andrade, S. E., Fouayzi, H. & Chan, K. A. Comparison of drug adherence rates among patients with seven different medical conditions. Pharmacotherapy 28, 437–443 (2008). [17]: Cutler, R. L., Fernandez-Llimos, F., Frommer, M., Benrimoj, C. & Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open 8, e016982 (2018).